Reimagining Healthcare Training with Augmented Reality (AR)
Clinical training in healthcare is expensive, contact-intensive, and difficult to scale. As the solo product designer on IQVIA's Apollo XR initiative, I led the end-to-end UX design of an augmented reality training application for Oculus devices, enabling nurses to practice complex medical procedures in immersive 3D environments, across locations, without a physical Clinical Research Associate present.
Keywords: Augmented Reality (AR) · Healthcare · UX · Clinical Training · Immersive Experience Design · User Onboarding · MVP · Scoping Medical Simulation · Enterprise
Client
Type
Year

Approach
Context
Business context: IQVIA, a global healthcare data and technology company, identified augmented reality as a strategic lever to reduce the cost and friction of clinical training. The Apollo XR app was its first of its kind into immersive AR, targeting nurses and healthcare professionals in institutional settings.
Team and role: I was the sole product designer embedded in a cross-functional team: a product owner, a product strategist, and developers. I owned all UX, from user research framing through wireframes, persona development, sitemap, and MVP definition.
Key constraints: The primary device was Oculus Quest 2, an emerging platform with limited design precedent in healthcare. We were working within regulatory considerations for medical software, with no existing AR UX patterns to borrow from. Timeline pressure meant we needed a clear MVP scope early.
The Problem
Clinical training for nurses is costly, requires in-person facilitators (CRAs), and is difficult to standardize across North America. Healthcare institutions needed a way to practice high-stakes procedures, like emergency response, without physical risk or logistical overhead.
Previous solutions were either passive video-based training or in-person simulation labs, neither of which scaled or offered meaningful interactivity. The risk: nurses entering high-pressure situations without sufficient hands-on preparation.
Approach
I defined success as: a nurse can complete a training session independently, understand where they are in the experience, and walk away with measurable competency data, all without a CRA in the room.
I deliberately scoped out social and gamification features, avatar customization, and mobile companion screens for MVP, focusing instead on orientation, navigation clarity, and a training loop that worked without prior AR experience. The strategic bet was that onboarding quality would determine whether the product lived or died in a clinical setting.
To align the team, I facilitated a prioritization session that mapped features against a Must/Should/Could/Won't framework, which gave the product owner and developer a shared decision boundary.
Process
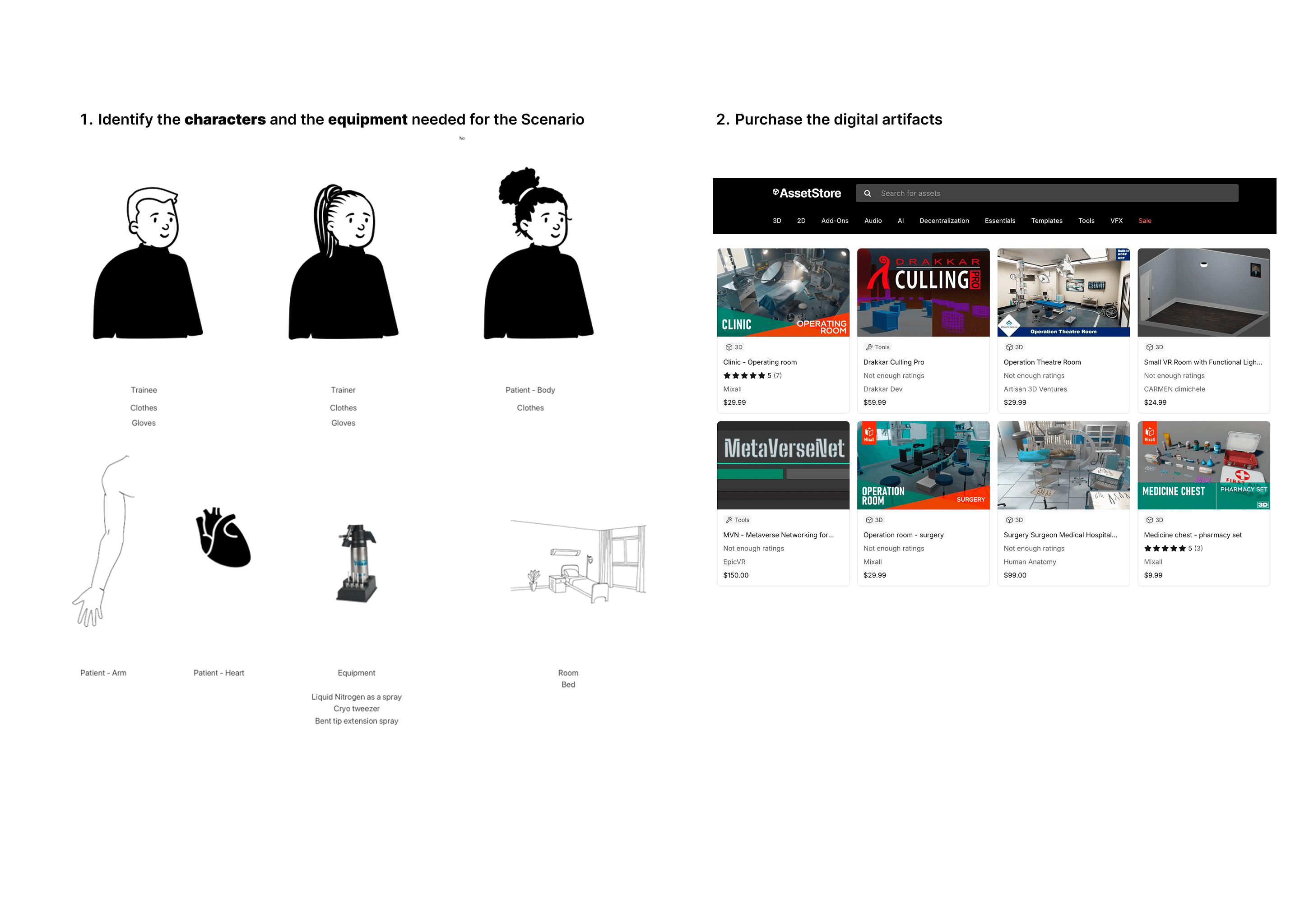
Research reframe: Early assumptions treated nurses as tech-savvy users. Interviews and persona work revealed two distinct user types, a clinical trainer and a trainee nurse, with very different mental models. This shifted the architecture significantly: trainers needed facilitation controls, trainees needed guided orientation.
Killing a scope creep: For instance the team pushed for Zoom integration and group chat early. I mapped these against the core training loop and showed they added complexity without improving the primary use case. Both were moved to the "Won't Have" column.
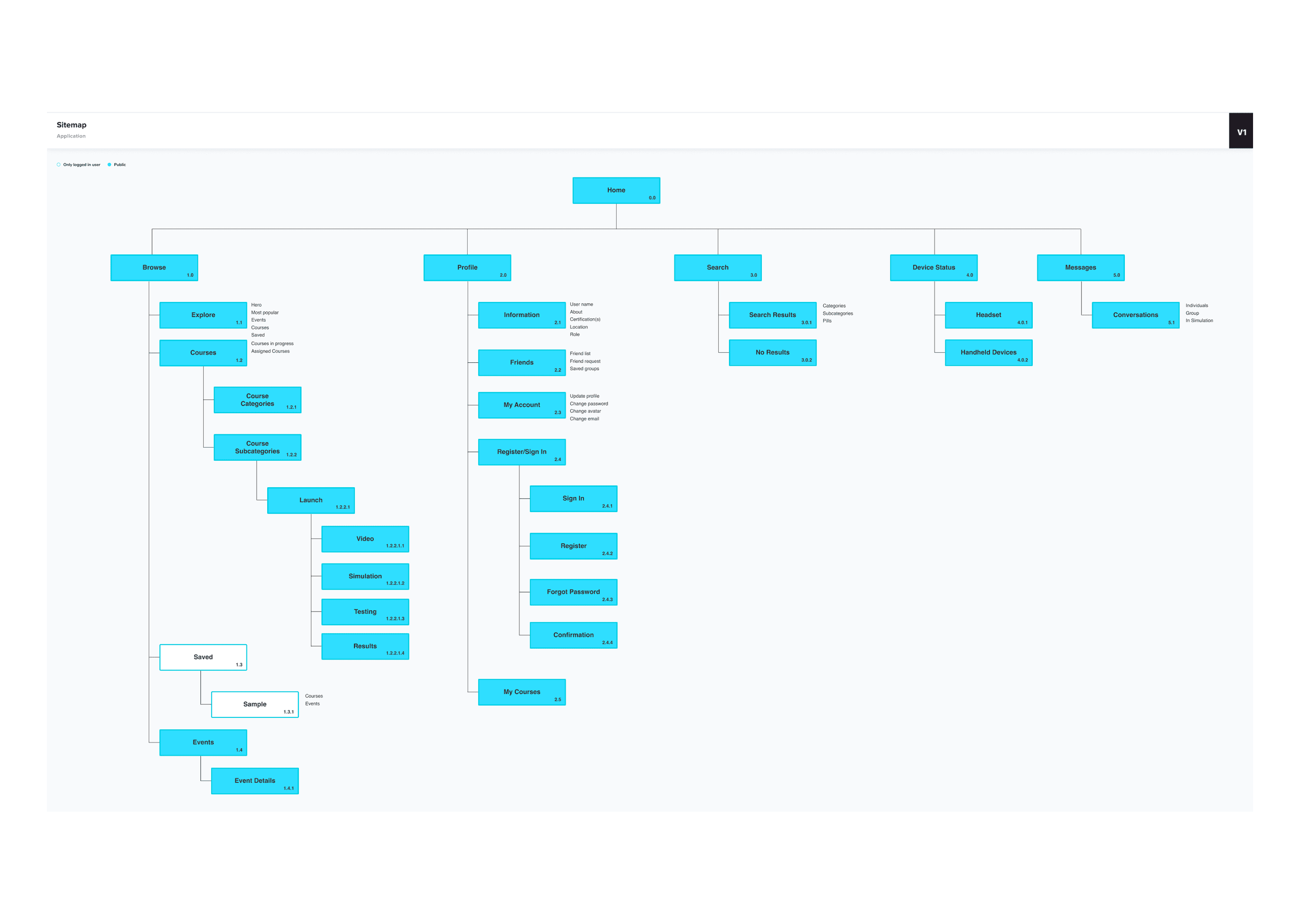
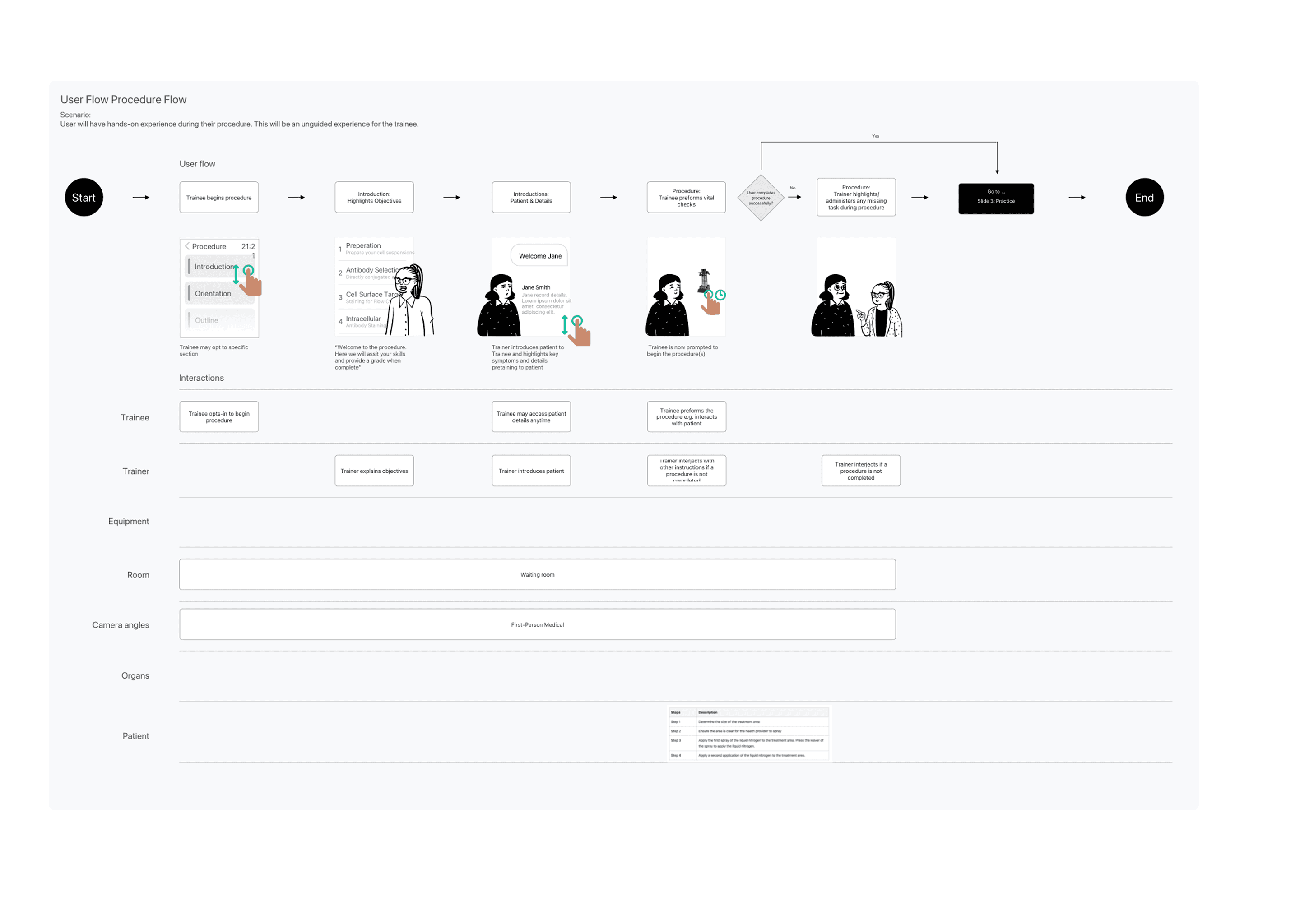
Sitemap and flow: I built a full sitemap covering onboarding, orientation, course selection, simulation entry, in-sim interactions (picking up objects, walking, procedures), and results review. This became the team's shared source of truth.
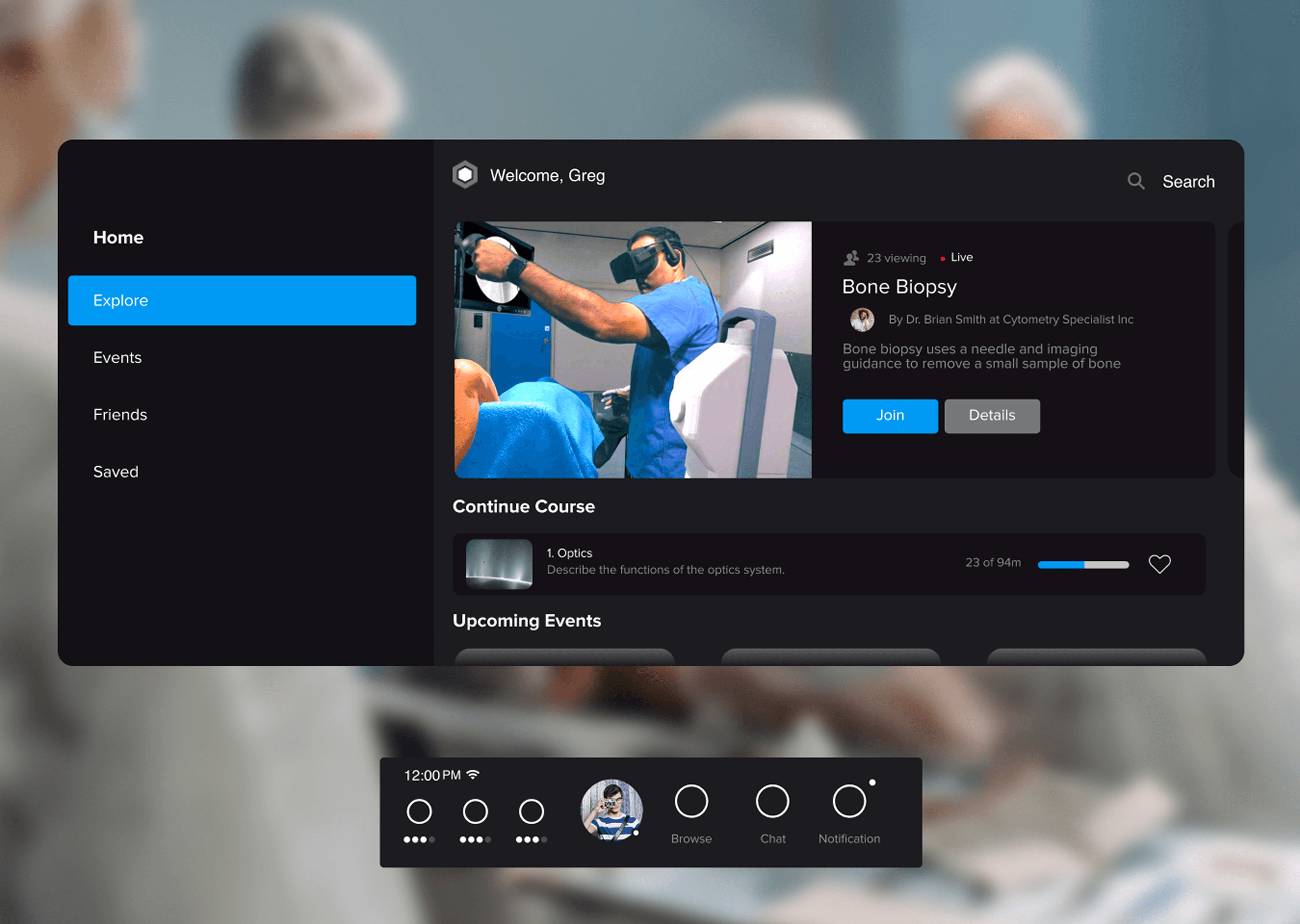
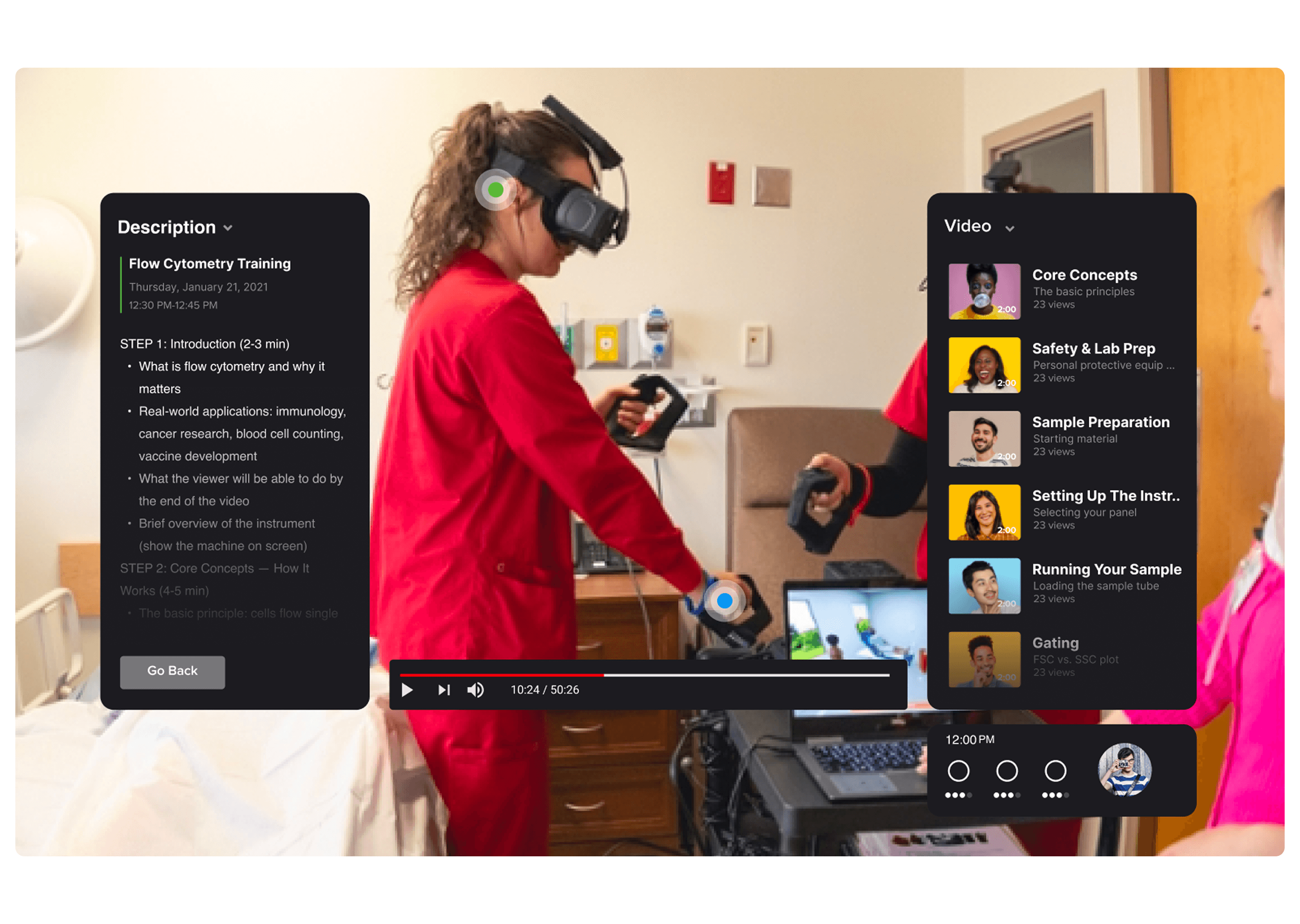
Wireframe iteration: Low-fi wireframes exposed a major gap: users had no persistent sense of location or progress inside the VR environment. I introduced a persistent Heads-Up Dashboard (HUD) with navigation, training status, and notifications, modeled loosely on game HUD conventions adapted for clinical UX.
Solution
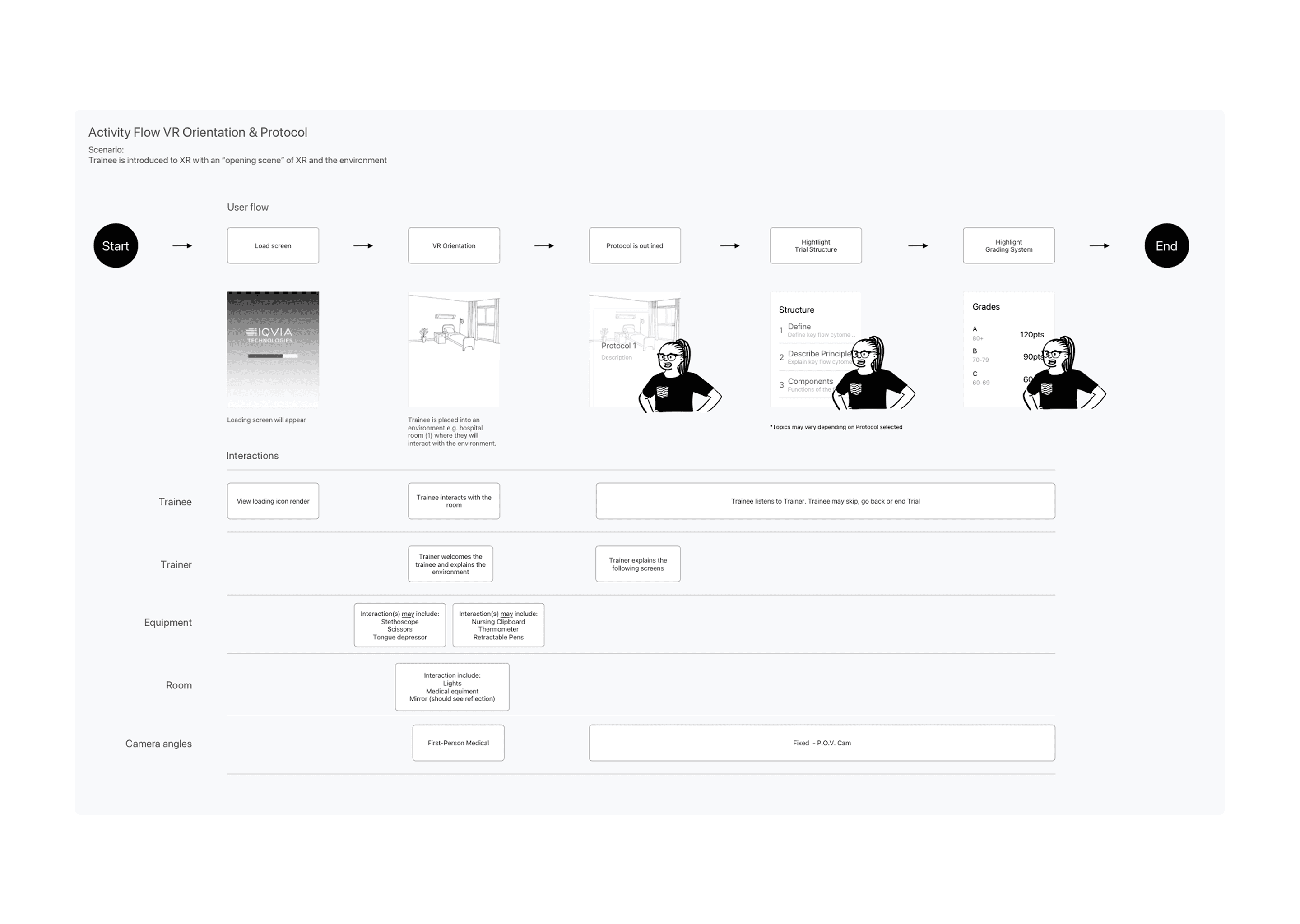
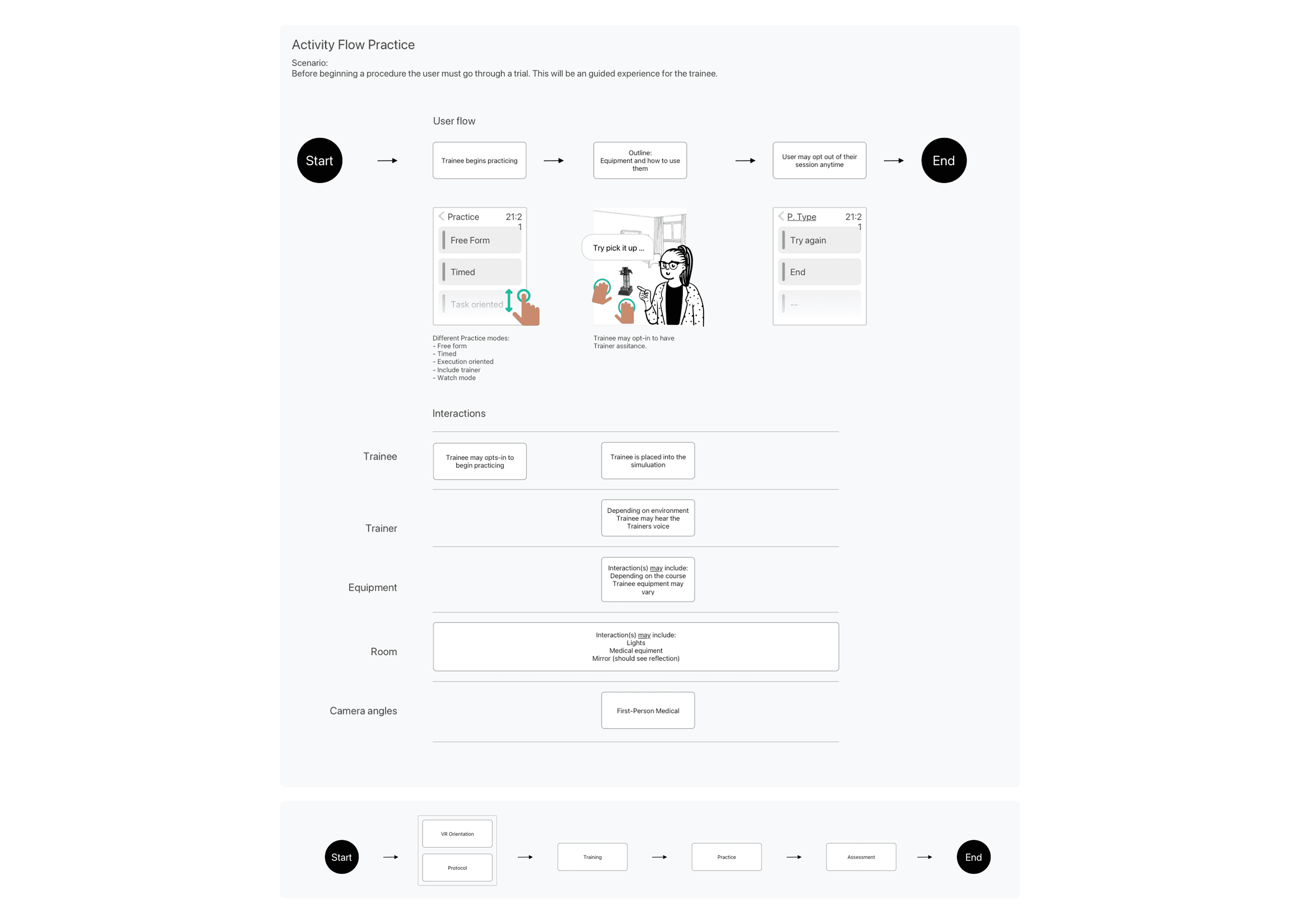
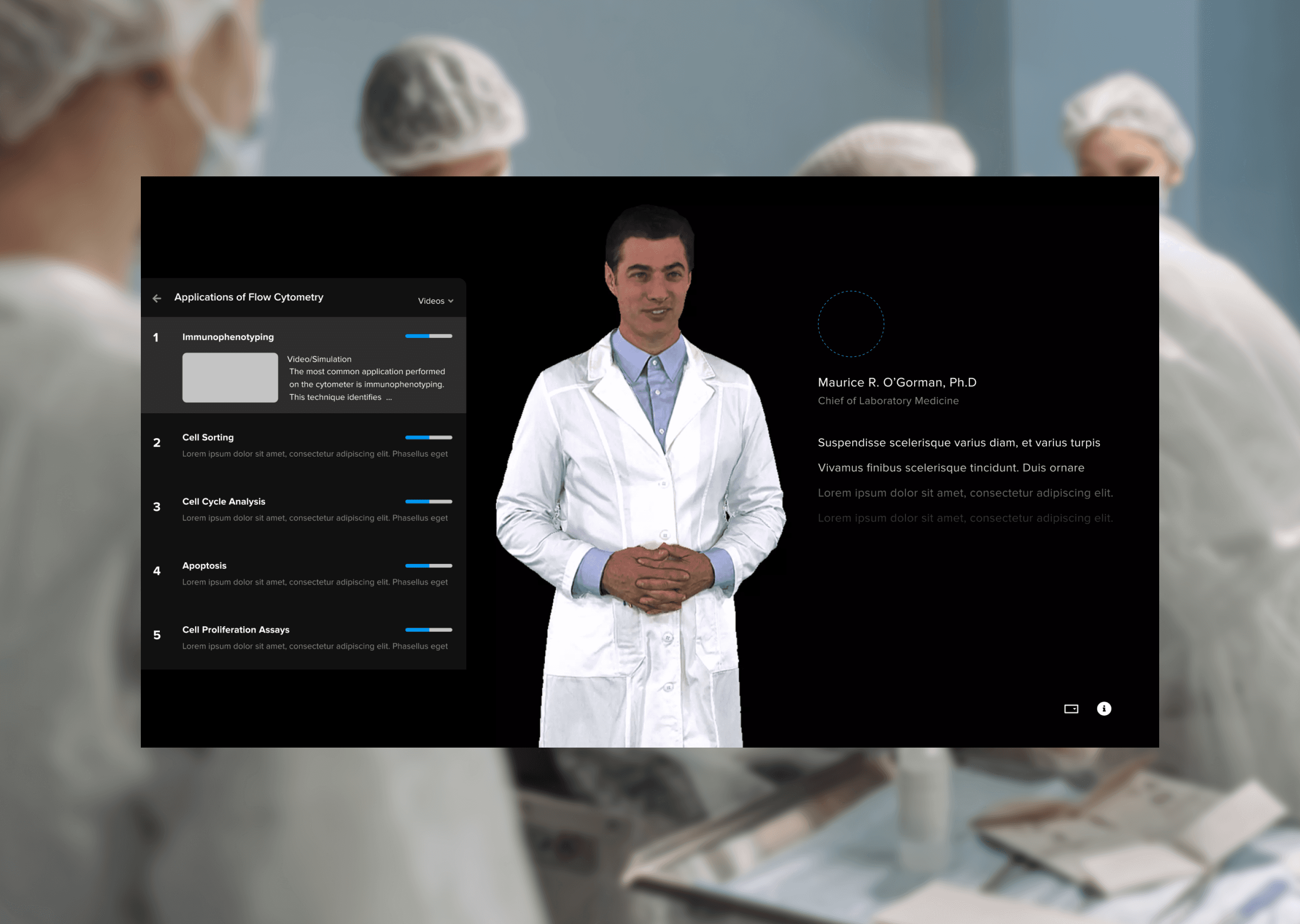
The core flow: a nurse loads the app, is oriented to the VR environment, selects a training simulation, practices a medical procedure guided by a trainer (live or async), and reviews pass/fail outcomes with competency data visualized post-session.
The highest-impact design decision was a structured onboarding sequence that oriented users to both the device and the application before any simulation began, removing the CRA dependency for first-time users.
Reflection
Outcome
Defined an MVP scope that reduced build complexity by cutting three premature feature sets
Delivered a sitemap, persona framework, and complete wireframes that became the development reference
Validated the training loop design within Oculus Quest 2 constraints in collaboration with engineering
Received stakeholder feedback describing the UX framework as “the clearest articulation of the product to date”
Reflection
Designing AR for a regulated space no direct comparators forced me to think from first principles. I realized that in unfamiliar environments, onboarding effectively is the product. Looking back, I would prioritize early usability testing with nurses in simulated headset conditions. This experience reshaped my approach to constraint-driven design: when users are navigating a new platform, minimizing cognitive load becomes the most impactful UX decision.

